218:
X-ray, however, does not exclude a diagnosis of thoracic aortic injury. A chest X-ray can also be useful to diagnose subsequent problems caused by aortic rupture such as pneumothorax or hemothorax. Non contrasted CT scans might show an intimal flap, periaortic hematoma, luminal filling defect, aortic contour abnormality, pseudoaneurysm, contained rupture, vessel wall disruption, active extravasation of intravenous contrast from the aorta and is therefore useful to assess for minimal aortic injury. Trans esophageal echos are useful in patients that are hemodynamically unstable, but the sensitivity and specificity of this study varies based on clinical user. The trans esophageal echo relies on placement an ultrasound probe into the patient's esophagus in order to get an ultrasound of the heart. If esophageal injury is expected, the patient has a facial injury, or if the patient has difficulty maintaining their away then the trans esophageal echo is contraindicated.
214:
imaging modality is CT angiogram which has a sensitivity of 100%. A CT angiogram relies on timing the CT scan after a bolus of IV contrast is administered from a peripheral IV site. Since a CT angiogram has a sensitivity of 100% and less invasive due to the peripheral placement of the IV line than aortagraphy it is the primary imaging choice. This allows visualization of the aorta and provides precise locations of traumatic injury. A CT angiogram does show both direct and indirect signs of aortic injury. The indirect sign that you can see is effacement of fat due to a hematoma. This sign should clue in a radiologist that there is an underlying injury. Some direct signs from a CT include having an intimal flap, irregularity of the shape of the aorta, filling defects secondary to a thrombus, or out pouching of the aorta.
68:. There are different grades to injuries to the aorta depending on the extent of injury, and the treatment whether surgical or medical depends on that grade. It is difficult to determine if a patient has a thoracic injury just by their symptoms, but through imaging and a physical exam the extent of injury can be determined. All patients with a thoracic aortic injury need to be treated either surgically with endovascular repair or open surgical repair or with medicine to keep their blood pressure and heart rate in the appropriate range. However, most patients that have a thoracic aortic injury do not live for 24 hours.
292:
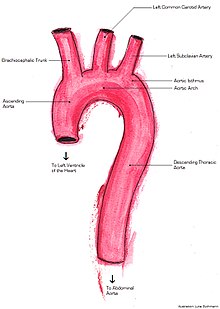
most common location followed by the portion of the aorta after the origin of the left subclavian artery. The most common mechanism leading to thoracic aortic injury is a motor vehicle collision. Other mechanisms include airplane crashes, falling from a large height and landing on a hard surface, or any injury that causes substantial pressure to the sternum. The incidence of thoracic aortic injuries is approximately 1 in 100,000.
105:(the portion of the aorta which is almost vertical), one mechanism of injury is torsion (a two-way twisting). There are clinical predictors of an aortic injury. The predictors include if a patient is older than 50, was an unrestrained patient, has hypotension, has a thoracic injury requiring thoracotomy, has a spinal injury, or has a head injury. If four of these criteria are met their likelihood for an aortic injury is 30%
29:
147:
might be external signs such as bruising on the anterior chest wall due to a traumatic injury. Clinical signs are uncommon and nonspecific but can include generalized hypertension due to the injury involving the sympathetic afferent nerves in the aortic isthmus. A murmur can also be audible as turbulent blood flow goes over the tear.
291:
Thoracic aortic injury is most commonly caused by a penetrating trauma in up to 90% of cases. Of these cases around 28% are confined to the thoracic portion of the aorta including the ascending aorta, aorta arch, and the descending aorta. Of the thoracic aortic injuries the ligament arteriosum is the
282:
Thoracic aortic injury is the 2nd leading cause of death involving both blunt trauma. 80% of patients that have a thoracic aortic injury will die immediately. Of the patients that do make it to be evaluated only 50% will survive 24 hours. Of the patients that do survive the first 24 hours 14% develop
108:
The aortic wall is made up of three different components the inner layer (intima), the muscle layer (media), and the outer layer (adventitia). A traumatic injury to the thoracic aorta can cause disruption of any of these parts. Therefore, aortic injury is on a scale from injury to a part of the inner
260:
Surgical repair is done by way of a thoracotomy or opening of the chest wall. From this point multiple methods can be used, but the most successful methods enable distal perfusion to prevent ischemia. When the surgery is performed a constant check of blood flow to the parts of the body away from the
273:
If the patient has minimal aortic injury then the patient can be managed non surgically. Rather the patient can be followed with serial images. If the patient does develop a more severe injury including a full thickness injury through the media layer then the patient should be treated with surgery.
230:
Due to the constant risk of sudden rupture or exsanguination urgent treatment is necessary. A patient can either undergo endovascular repair or surgical repair. Endovascular repair is the current gold standard due to increased success rates and lower complications. Patients that are able to undergo
217:
However, non contrasted CT scans, chest X-rays, and transesophageal echos can also be used. Chest X-rays most sensitive finding is a widened mediastinum of greater than 8 cm. An apical cap and displacement of the trachea to either side of the chest from midline can also be seen. A normal chest
213:
The gold standard for diagnosis of thoracic aortic injury is aortography. This method involves inserting a catheter into the aorta and directly injecting contrast material. The primary benefit of aortography is the ability to precisely determine the location of injury for surgical planning. Another
129:
In addition to the 4 grades of aortic injury, the risk of rupture can also be categorized. If both the inner layer and the muscle layer of the aortic wall are both involved in the injury then the injury is categorized as significant aortic injury. If just the inner layer and a portion of the muscle
133:
Between the mobile ascending aorta and the relatively fixed descending thoracic aorta is the aortic isthmus. When there is a sudden deceleration the mobile ascending aorta pushes forward creating a whiplash effect on the aortic isthmus. However, a different mechanism is involved when the ascending
146:
It is difficult to rely on symptoms to diagnose a thoracic aortic injury. However some symptoms do include severe chest pain, cough, shortness of breath, difficulty swallowing due to compression of the esophagus, back pain, and hoarseness due to involvement of the recurrent laryngeal nerve. There
269:
While waiting for surgery careful regulation of blood pressure and heart rate is necessary. Systolic blood pressure should be maintained between 100 and 120 mmHg allowing for perfusion distal to the injury but decreasing the risk of rupture while the heart rate should be kept under 100 beats per
226:
The first line treatment for patients with thoracic aortic injury is maintaining the patient's airway with intubation and treating secondary injuries such as a hemothorax. After ensuring the patient has a patent airway and other life-threatening injuries are treated then treatment for the aortic
137:
Based on the location of the injury in the thorax subsequent injuries can take place. If the injury is in the descending thoracic aorta this could lead to a hemothorax. Where as an injury to the ascending aorta could lead to hemoperricardium and subsequent tamponade or could compress the SVC.
270:
minute. Esmolol is first choice to maintain blood pressure and heart rate due to its short time of action, but if the blood pressure is not within range adding nitroprusside sodium can be added as a second agent. The treatment is similar to what is done for aortic dissections.
245:
Endovascular repair is done by first gaining vascular access usually through the femoral artery. A catheter is inserted to the point of injury and a luminal stent is deployed. Blood is then able to be pumped through the stent and prevent the aortic wall from rupturing.
134:
aorta proximal to the isthmus is torn. When there is a rapid deceleration the heart is pushed to the left posterior chest. This causes a sudden increase in intra-aortic pressure and can cause aortic rupture. This is known as the water hammer effect.
204:
as they believe it implies that a tear is incompatible with life; however, the term accurately gauges the severity of tears in the aorta. A rupture can be either complete or partial, and can be classified further by the position of the tear.
925:
910:
84:
and falls from a substantial height. Several mechanical processes can occur and are reflected in the injury itself. A more recently proposed mechanism is that the aorta can be compressed between bony structures (such as the
231:
endovascular repair without contraindications should proceed with it. Repair should be delayed if there is life-threatening intra-abdominal or intracranial bleeding or if the patient is at risk for infection.
130:
layer are involved in the injury then the injury is characterized as minimal aortic injury. Radiographically this would be seen as an intimal flap less than 1 cm in size.
873:
816:
741:
672:
619:
453:
400:
1277:
160:
There are inconsistencies in the terminology of aortic injury. There are several terms which are interchangeably used to describe injury to the aorta such as
1007:
849:
792:
717:
648:
595:
502:
429:
376:
1607:
424:. Markovchick, Vincent J.,, Pons, Peter T.,, Bakes, Katherine M.,, Buchanan, Jennie A. (Sixth ed.). Philadelphia, PA. 2015-11-10.
1612:
1168:
1663:
322:
Lee, W. Anthony; Matsumura, Jon; Mitchell, R. Scott; Farber, Mark; Greenburg, Roy; Murad, Mohammad; Fairman, Ronald (2011).
324:"Endovascular repair of traumatic thoracic aortic injury: Clinical practice guidelines of the Society for Vascular Surgery"
1304:
1272:
240:
1000:
877:
820:
745:
676:
623:
526:
457:
404:
1627:
1345:
787:. Walls, Ron M.,, Hockberger, Robert S.,, Gausche-Hill, Marianne (Ninth ed.). Philadelphia, PA. 2017-03-09.
1241:
1233:
1045:
189:
1472:
1467:
1130:
1096:
1668:
1477:
1314:
1309:
81:
80:
and crush injuries. Deceleration injuries almost always occur during high speed impacts, such as those in
1694:
1656:
1402:
1246:
1216:
1135:
993:
643:. Gropper, Michael A., 1958-, Miller, Ronald D., 1939- (Ninth ed.). Philadelphia, PA. 2019-10-07.
371:. Digumarthy, Subba R. (Subba Rao),, Abbara, Suhny,, Chung, Jonathan H. Philadelphia, PA. March 2019.
192:. For all intents and purposes, the latter is used when a tear occurs across all or nearly all of the
1617:
1256:
1161:
1125:
1065:
543:
Creasy JD, Chiles C, Routh WD, Dyer RB (1997). "Overview of traumatic injury of the thoracic aorta".
60:; however, they can also be the result of a pathological process. The main causes of this injury are
1452:
1422:
1120:
929:
255:
1587:
1566:
1525:
1392:
1084:
1030:
867:
810:
735:
666:
613:
520:
447:
394:
1699:
1437:
1432:
1387:
1074:
962:
855:
845:
798:
788:
723:
713:
654:
644:
601:
591:
560:
508:
498:
435:
425:
382:
372:
345:
1582:
1546:
1115:
590:. Walker, Christopher M.,, Chung, Jonathan H. (2nd ed.). Philadelphia, PA. 2018-08-17.
552:
335:
185:
98:
1154:
1079:
1069:
102:
57:
1639:
1634:
1457:
1324:
556:
44:
938:
1688:
1673:
1556:
1520:
1515:
1377:
1319:
1211:
1020:
193:
985:
934:
844:. Sidawy, Anton N.,, Perler, Bruce A. (9th ed.). Philadelphia, PA. 2018-04-03.
1651:
1551:
1510:
1500:
1495:
1417:
1201:
1196:
1105:
1016:
973:
77:
65:
61:
53:
497:. Adams, James, 1962- (2nd ed.). Philadelphia, Pa: Elsevier/ Saunders. 2013.
1622:
1561:
1407:
1329:
1060:
957:
200:
is defined as a forcible disruption of tissue. Some disagree with the usage of
1530:
1412:
1251:
1191:
1110:
919:
859:
727:
658:
605:
386:
340:
323:
802:
512:
439:
1382:
968:
86:
349:
28:
712:. Bersten, Andrew D.,, Handy, Jonathan M. (Eighth ed.). 2018-08-15.
564:
1646:
1040:
90:
902:
1366:
1206:
1177:
914:
49:
1505:
785:
Rosen's emergency medicine : concepts and clinical practice
261:
injury should be monitored to know if oxygenation is occurring.
76:
Injuries to the aorta are usually the result of trauma, such as
1150:
989:
94:
180:
is used as a term for the consequence of a tear, whereas a
56:. Injuries of the thoracic aorta are usually the result of
1146:
842:
Rutherford's vascular surgery and endovascular therapy
48:
refers to any injury which affects the portion of the
892:
1600:
1575:
1539:
1488:
1365:
1358:
1338:
1297:
1290:
1265:
1232:
1225:
1184:
1093:
1027:
948:
896:
21:
109:layer to a complete tear of all three layers.
1278:Focused assessment with sonography for trauma
1162:
1001:
495:Emergency medicine : clinical essentials
8:
1362:
1294:
1229:
1169:
1155:
1147:
1008:
994:
986:
893:
872:: CS1 maint: location missing publisher (
815:: CS1 maint: location missing publisher (
740:: CS1 maint: location missing publisher (
671:: CS1 maint: location missing publisher (
618:: CS1 maint: location missing publisher (
538:
536:
452:: CS1 maint: location missing publisher (
399:: CS1 maint: location missing publisher (
27:
18:
339:
301:
865:
808:
733:
664:
611:
518:
445:
392:
112:There are 4 grades of aortic injury.
836:
834:
832:
830:
779:
777:
775:
489:
487:
7:
773:
771:
769:
767:
765:
763:
761:
759:
757:
755:
704:
702:
700:
698:
696:
694:
692:
690:
688:
686:
635:
633:
582:
580:
578:
576:
574:
485:
483:
481:
479:
477:
475:
473:
471:
469:
467:
416:
414:
363:
361:
359:
317:
315:
313:
311:
309:
307:
305:
1608:Acute respiratory distress syndrome
557:10.1148/radiographics.17.1.9017797
14:
1613:Chronic traumatic encephalopathy
369:Problem solving in chest imaging
1664:Post-traumatic stress disorder
1:
588:Müller's imaging of the chest
64:(such as a car accident) and
36:Anatomy of the thoracic aorta
1305:Advanced trauma life support
1273:Diagnostic peritoneal lavage
241:Endovascular aneurysm repair
119:Type II: Intramural hematoma
328:Journal of Vascular Surgery
1716:
710:Oh's intensive care manual
422:Emergency medicine secrets
253:
238:
1346:Resuscitative thoracotomy
1234:Clinical prediction rules
341:10.1016/j.jvs.2010.08.027
35:
26:
1242:Abbreviated Injury Scale
1046:Traumatic aortic rupture
122:Type III: Pseudoaneurysm
1473:Penetrating head injury
1468:Intracranial hemorrhage
1131:Tracheobronchial injury
1097:lower respiratory tract
227:injury can be started.
184:is a section across an
1669:Subcutaneous emphysema
1628:Volkmann's contracture
1478:Traumatic brain injury
1315:Early appropriate care
1310:Damage control surgery
525:: CS1 maint: others (
52:which lies within the
1443:Thoracic aorta injury
1403:Diaphragmatic rupture
1247:Injury Severity Score
1217:Trauma triad of death
1136:Diaphragmatic rupture
1051:Thoracic aorta injury
876:) CS1 maint: others (
819:) CS1 maint: others (
744:) CS1 maint: others (
675:) CS1 maint: others (
622:) CS1 maint: others (
456:) CS1 maint: others (
403:) CS1 maint: others (
82:motor vehicle crashes
22:Thoracic aorta injury
1618:Compartment syndrome
1257:Revised Trauma Score
1126:Pulmonary laceration
1066:Myocardial contusion
250:Open Surgical Repair
116:Type I: Intimal tear
1453:Blunt kidney trauma
1423:Pulmonary contusion
1121:Pulmonary contusion
641:Miller's anesthesia
256:Open aortic surgery
235:Endovascular Repair
1567:Spinal cord injury
1526:Penetrating trauma
1393:Soft tissue injury
1085:Myocardial rupture
1031:circulatory system
949:External resources
265:Medical Management
1682:
1681:
1596:
1595:
1438:Internal bleeding
1433:Cardiac tamponade
1388:Joint dislocation
1354:
1353:
1286:
1285:
1144:
1143:
1075:Cardiac tamponade
983:
982:
851:978-0-323-58130-1
794:978-0-323-39016-3
719:978-0-7020-7606-0
650:978-0-323-61264-7
597:978-0-323-53179-5
504:978-1-4377-3548-2
431:978-0-323-37483-5
378:978-0-323-04132-4
40:
39:
16:Medical condition
1707:
1588:Pediatric trauma
1583:Geriatric trauma
1547:Abdominal trauma
1363:
1295:
1230:
1171:
1164:
1157:
1148:
1116:Hemopneumothorax
1010:
1003:
996:
987:
894:
882:
881:
871:
863:
838:
825:
824:
814:
806:
781:
750:
749:
739:
731:
706:
681:
680:
670:
662:
637:
628:
627:
617:
609:
584:
569:
568:
540:
531:
530:
524:
516:
491:
462:
461:
451:
443:
418:
409:
408:
398:
390:
365:
354:
353:
343:
319:
125:Type IV: Rupture
31:
19:
1715:
1714:
1710:
1709:
1708:
1706:
1705:
1704:
1685:
1684:
1683:
1678:
1592:
1571:
1535:
1484:
1359:Pathophysiology
1350:
1334:
1282:
1261:
1221:
1180:
1175:
1145:
1140:
1095:
1089:
1080:Hemopericardium
1070:Commotio cordis
1029:
1023:
1014:
984:
979:
978:
944:
943:
905:
891:
886:
885:
864:
852:
840:
839:
828:
807:
795:
783:
782:
753:
732:
720:
708:
707:
684:
663:
651:
639:
638:
631:
610:
598:
586:
585:
572:
542:
541:
534:
517:
505:
493:
492:
465:
444:
432:
420:
419:
412:
391:
379:
367:
366:
357:
321:
320:
303:
298:
289:
280:
267:
258:
252:
243:
237:
224:
211:
158:
153:
144:
103:ascending aorta
74:
58:physical trauma
17:
12:
11:
5:
1713:
1711:
1703:
1702:
1697:
1687:
1686:
1680:
1679:
1677:
1676:
1671:
1666:
1661:
1660:
1659:
1654:
1644:
1643:
1642:
1640:Rhabdomyolysis
1635:Crush syndrome
1632:
1631:
1630:
1620:
1615:
1610:
1604:
1602:
1598:
1597:
1594:
1593:
1591:
1590:
1585:
1579:
1577:
1573:
1572:
1570:
1569:
1564:
1559:
1554:
1549:
1543:
1541:
1537:
1536:
1534:
1533:
1528:
1523:
1518:
1513:
1508:
1503:
1498:
1492:
1490:
1486:
1485:
1483:
1482:
1481:
1480:
1475:
1470:
1462:
1461:
1460:
1458:Splenic injury
1455:
1447:
1446:
1445:
1440:
1435:
1427:
1426:
1425:
1420:
1415:
1410:
1405:
1397:
1396:
1395:
1390:
1385:
1380:
1371:
1369:
1360:
1356:
1355:
1352:
1351:
1349:
1348:
1342:
1340:
1336:
1335:
1333:
1332:
1327:
1325:Trauma surgery
1322:
1317:
1312:
1307:
1301:
1299:
1292:
1288:
1287:
1284:
1283:
1281:
1280:
1275:
1269:
1267:
1266:Investigations
1263:
1262:
1260:
1259:
1254:
1249:
1244:
1238:
1236:
1227:
1223:
1222:
1220:
1219:
1214:
1209:
1204:
1199:
1194:
1188:
1186:
1182:
1181:
1176:
1174:
1173:
1166:
1159:
1151:
1142:
1141:
1139:
1138:
1133:
1128:
1123:
1118:
1113:
1108:
1102:
1100:
1091:
1090:
1088:
1087:
1082:
1077:
1072:
1056:
1055:
1054:
1053:
1036:
1034:
1025:
1024:
1015:
1013:
1012:
1005:
998:
990:
981:
980:
977:
976:
965:
953:
952:
950:
946:
945:
942:
941:
922:
906:
901:
900:
898:
897:Classification
890:
889:External links
887:
884:
883:
850:
826:
793:
751:
718:
682:
649:
629:
596:
570:
532:
503:
463:
430:
410:
377:
355:
334:(1): 187–192.
300:
299:
297:
294:
288:
285:
279:
276:
266:
263:
254:Main article:
251:
248:
239:Main article:
236:
233:
223:
220:
210:
207:
196:of the aorta.
157:
156:Classification
154:
152:
149:
143:
140:
127:
126:
123:
120:
117:
73:
70:
66:crush injuries
45:thoracic aorta
43:Injury of the
38:
37:
33:
32:
24:
23:
15:
13:
10:
9:
6:
4:
3:
2:
1712:
1701:
1698:
1696:
1693:
1692:
1690:
1675:
1674:Wound healing
1672:
1670:
1667:
1665:
1662:
1658:
1655:
1653:
1650:
1649:
1648:
1645:
1641:
1638:
1637:
1636:
1633:
1629:
1626:
1625:
1624:
1621:
1619:
1616:
1614:
1611:
1609:
1606:
1605:
1603:
1601:Complications
1599:
1589:
1586:
1584:
1581:
1580:
1578:
1574:
1568:
1565:
1563:
1560:
1558:
1557:Facial trauma
1555:
1553:
1550:
1548:
1545:
1544:
1542:
1538:
1532:
1529:
1527:
1524:
1522:
1521:Gunshot wound
1519:
1517:
1516:Electrocution
1514:
1512:
1509:
1507:
1504:
1502:
1499:
1497:
1494:
1493:
1491:
1487:
1479:
1476:
1474:
1471:
1469:
1466:
1465:
1463:
1459:
1456:
1454:
1451:
1450:
1448:
1444:
1441:
1439:
1436:
1434:
1431:
1430:
1428:
1424:
1421:
1419:
1416:
1414:
1411:
1409:
1406:
1404:
1401:
1400:
1398:
1394:
1391:
1389:
1386:
1384:
1381:
1379:
1378:Bone fracture
1376:
1375:
1373:
1372:
1370:
1368:
1364:
1361:
1357:
1347:
1344:
1343:
1341:
1337:
1331:
1328:
1326:
1323:
1321:
1320:Trauma center
1318:
1316:
1313:
1311:
1308:
1306:
1303:
1302:
1300:
1296:
1293:
1289:
1279:
1276:
1274:
1271:
1270:
1268:
1264:
1258:
1255:
1253:
1250:
1248:
1245:
1243:
1240:
1239:
1237:
1235:
1231:
1228:
1224:
1218:
1215:
1213:
1212:Resuscitation
1210:
1208:
1205:
1203:
1200:
1198:
1195:
1193:
1190:
1189:
1187:
1183:
1179:
1172:
1167:
1165:
1160:
1158:
1153:
1152:
1149:
1137:
1134:
1132:
1129:
1127:
1124:
1122:
1119:
1117:
1114:
1112:
1109:
1107:
1104:
1103:
1101:
1098:
1092:
1086:
1083:
1081:
1078:
1076:
1073:
1071:
1067:
1064:
1062:
1058:
1057:
1052:
1049:
1048:
1047:
1044:
1042:
1038:
1037:
1035:
1032:
1026:
1022:
1018:
1011:
1006:
1004:
999:
997:
992:
991:
988:
975:
971:
970:
966:
964:
960:
959:
955:
954:
951:
947:
940:
936:
932:
931:
927:
923:
921:
917:
916:
912:
908:
907:
904:
899:
895:
888:
879:
875:
869:
861:
857:
853:
847:
843:
837:
835:
833:
831:
827:
822:
818:
812:
804:
800:
796:
790:
786:
780:
778:
776:
774:
772:
770:
768:
766:
764:
762:
760:
758:
756:
752:
747:
743:
737:
729:
725:
721:
715:
711:
705:
703:
701:
699:
697:
695:
693:
691:
689:
687:
683:
678:
674:
668:
660:
656:
652:
646:
642:
636:
634:
630:
625:
621:
615:
607:
603:
599:
593:
589:
583:
581:
579:
577:
575:
571:
566:
562:
558:
554:
550:
546:
545:Radiographics
539:
537:
533:
528:
522:
514:
510:
506:
500:
496:
490:
488:
486:
484:
482:
480:
478:
476:
474:
472:
470:
468:
464:
459:
455:
449:
441:
437:
433:
427:
423:
417:
415:
411:
406:
402:
396:
388:
384:
380:
374:
370:
364:
362:
360:
356:
351:
347:
342:
337:
333:
329:
325:
318:
316:
314:
312:
310:
308:
306:
302:
295:
293:
286:
284:
277:
275:
271:
264:
262:
257:
249:
247:
242:
234:
232:
228:
221:
219:
215:
208:
206:
203:
199:
195:
194:circumference
191:
190:cross section
187:
183:
179:
175:
171:
167:
163:
155:
150:
148:
141:
139:
135:
131:
124:
121:
118:
115:
114:
113:
110:
106:
104:
100:
96:
92:
88:
83:
79:
71:
69:
67:
63:
59:
55:
51:
47:
46:
34:
30:
25:
20:
1695:Chest trauma
1552:Chest injury
1511:Crush injury
1501:Blunt trauma
1496:Blast injury
1442:
1418:Pneumothorax
1202:Traumatology
1197:Major trauma
1106:Pneumothorax
1059:
1050:
1039:
1019:, excluding
1017:Chest injury
967:
956:
924:
909:
841:
784:
709:
640:
587:
551:(1): 27–45.
548:
544:
494:
421:
368:
331:
327:
290:
287:Epidemiology
283:paraplegia.
281:
272:
268:
259:
244:
229:
225:
216:
212:
201:
197:
181:
177:
173:
169:
165:
161:
159:
145:
136:
132:
128:
111:
107:
93:, and first
78:deceleration
75:
62:deceleration
54:chest cavity
42:
41:
1623:Contracture
1576:Demographic
1562:Head injury
1408:Flail chest
1330:Trauma team
1028:Cardiac and
958:MedlinePlus
182:transection
170:transection
1689:Categories
1531:Stab wound
1413:Hemothorax
1339:Procedures
1298:Principles
1291:Management
1252:NACA score
1226:Assessment
1192:Polytrauma
1185:Principles
1111:Hemothorax
860:1037557259
728:1053859479
659:1124935549
606:1051135278
387:1126790420
296:References
178:Laceration
166:laceration
97:) and the
1489:Mechanism
1383:Degloving
1021:fractures
969:eMedicine
868:cite book
811:cite book
803:989157341
736:cite book
667:cite book
614:cite book
521:cite book
513:820203833
448:cite book
440:932082432
395:cite book
222:Treatment
151:Diagnosis
101:. In the
87:manubrium
72:Mechanism
1700:Injuries
1647:Embolism
1099:injuries
1094:Lung and
1041:vascular
1033:injuries
974:radio/44
350:20974523
278:Outcomes
142:Symptoms
91:clavicle
1429:Cardio
565:9017797
209:Imaging
202:rupture
198:Rupture
174:rupture
1540:Region
1464:Neuro
1367:Injury
1207:Triage
1178:Trauma
963:001062
858:
848:
801:
791:
726:
716:
657:
647:
604:
594:
563:
511:
501:
438:
428:
385:
375:
348:
172:, and
1399:Resp
1061:heart
939:901.0
920:S25.0
99:spine
50:aorta
1506:Burn
1374:MSK
930:9-CM
878:link
874:link
856:OCLC
846:ISBN
821:link
817:link
799:OCLC
789:ISBN
746:link
742:link
724:OCLC
714:ISBN
677:link
673:link
655:OCLC
645:ISBN
624:link
620:link
602:OCLC
592:ISBN
561:PMID
527:link
509:OCLC
499:ISBN
458:link
454:link
436:OCLC
426:ISBN
405:link
401:link
383:OCLC
373:ISBN
346:PMID
186:axis
162:tear
1657:fat
1652:air
1449:GI
935:441
926:ICD
911:ICD
553:doi
336:doi
188:or
95:rib
1691::
972::
961::
937:,
933::
918::
915:10
870:}}
866:{{
854:.
829:^
813:}}
809:{{
797:.
754:^
738:}}
734:{{
722:.
685:^
669:}}
665:{{
653:.
632:^
616:}}
612:{{
600:.
573:^
559:.
549:17
547:.
535:^
523:}}
519:{{
507:.
466:^
450:}}
446:{{
434:.
413:^
397:}}
393:{{
381:.
358:^
344:.
332:53
330:.
326:.
304:^
176:.
168:,
164:,
89:,
1170:e
1163:t
1156:v
1068:/
1063::
1043::
1009:e
1002:t
995:v
928:-
913:-
903:D
880:)
862:.
823:)
805:.
748:)
730:.
679:)
661:.
626:)
608:.
567:.
555::
529:)
515:.
460:)
442:.
407:)
389:.
352:.
338::
Text is available under the Creative Commons Attribution-ShareAlike License. Additional terms may apply.